

Adenozine Issue 1
Two Guidelines, One Condition? — ACS 2025

EDITOR’S NOTE
Welcome to the first issue of Adenozine!
This newsletter exists because keeping up with cardiac emergency evidence while working in a busy ED is genuinely hard. My aim is simple: cut through the noise and deliver what matters for frontline practice, in the time it takes to finish a coffee.
Everyone who works in Emergency Medicine knows this term and it’s a condition we meet on an almost daily basis, since chest pain is one of the most common presenting complaints to the ED and ACS is virtually always on the list…
Issue 1 felt like an obvious place to start (bah dum ching!). First, we have two major ACS guidelines to discuss that both landed in 2025: one from the US, one from home and they don’t always agree. Rather than summarizing them separately, I thought it was more useful to put them side by side and highlight where Australian practice should and shouldn’t follow the American lead.
For those who want a little more (and have a bit more time), there is a summary of what you need to know from the Australian ACS Guidelines included as well…
If there’s a topic or paper you’d like covered in a future issue, hit reply. I’d genuinely love to hear from you.
Joe Rotella Emergency Physician, Clinical Toxicologist, and Cardiac Emergency Research Lead (Victorian Heart Hospital)
Why this matters for Australian ED physicians?
Two landmark ACS guidelines landed in 2025 - one from the US, one from home. Both synthesize the same evidence base, but they don’t always reach the same conclusions. Here’s what you need to know…
1. A new name for an old pattern
The Australian guideline introduces a term the US guideline doesn’t use: ACOMI or Acute Coronary Occlusion Myocardial Infarction. This deliberately broadens the STEMI concept to capture posterior MI, De Winter’s T-waves, and right ventricular infarction patterns. These are ECG findings that represent acute occlusion but don’t meet the traditional STE criteria.
A more in-depth summary can be found below.
The clinical implication is the same in both guidelines (emergency reperfusion), but Australia’s framing better reflects the biology. Worth knowing if colleagues, ED or Cardiology, are using this language.
2. Time is cardiac muscle! STEMI reperfusion timing
The Australian Guidelines recommend a stricture window for reperfusion- <60 min from first hospital arrival at a PCI-capable centre and <90 min following transfer from a non-PCI centre. In contrast, the US Guidelines recommend less than or equal to 90 minutes and 120 minutes respectivelly.
If your cath lab in Australia isn’t hitting 60 minutes door-to-balloon, this guideline wants to a ‘please explain’…
3. Half-dose tenecteplase in the elderly
For patients aged ≥70 years receiving fibrinolysis, the Australian guideline gives an explicit strong recommendation for half-dose tenecteplase as part of a pharmaco-invasive strategy. The US guideline notes tenecteplase is preferred but doesn’t stratify by age in the same way.
This matters in regional Australian settings where lytic therapy is the realistic reperfusion option.
4. DAPT duration - more flexibility Down Under
The US guideline defaults to 12 months of DAPT (dual anti-platelet therapy). The Australian guideline takes a more stratified approach:
High ischaemic / low bleeding risk: 6–12 months DAPT
Low ischaemic / high bleeding risk: cease DAPT at 1–3 months, continue single antiplatelet
This is clinically useful — the Australian algorithm acknowledges that one size does not fit all and gives the ED physician and cardiologist a framework for shared decision-making at discharge.
Bottom line for Australian ED physicians
The two guidelines are broadly aligned on the major pillars — radial access, radial over femoral, hs-troponin CDPs, potent P2Y12 inhibitors in PCI-managed ACS.
Where they diverge is often where the Australian context matters most: stricter reperfusion timing, age-specific fibrinolytic dosing, and a more nuanced DAPT algorithm.
The Australian guideline also has a stronger equity focus, with specific guidance for First Nations patients that the US guideline does not replicate.
Read both. Apply the one that fits where you work.
QUALITY FLAG

Both documents reviewed in this issue are society-level clinical practice guidelines developed using GRADE methodology, incorporating systematic literature review to approximately mid-2024. Neither represents primary trial data.
The Australian guideline was jointly funded by the Heart Foundation and CSANZ with no commercial sponsorship.
The US guideline was developed without commercial support by the ACC/AHA, with co-endorsement from ACEP, NAEMSP and SCAI, making it one of the few major cardiology guidelines with formal emergency medicine input.
Recommendations from both documents should be interpreted alongside local resources, system capabilities and individual patient circumstances.
So now that we’ve compared apples, let’s take a bite of the Aussie one…
The 2025 Australian ACS Guidelines: What You Actually Need to Know in the ED
Brieger et al., Heart Lung Circ 2025 — NHF/CSANZ Comprehensive Australian Clinical Guideline for Diagnosing and Managing Acute Coronary Syndromes
At 137 pages, nobody’s reading this cover to cover on a night shift. Here’s what matters…
The ACOMI Rebrand
The biggest conceptual shift in this guideline is the introduction of ACOMI — Acute Coronary Occlusion Myocardial Infarction. It’s not just a new acronym. It’s a deliberate expansion beyond classic STEMI criteria to capture every ECG pattern representing an acutely occluded vessel. If there’s occlusion, the reperfusion pathway opens — regardless of whether traditional STE criteria are met.
The guideline formalizes the following as ACOMI-equivalent patterns warranting activation:
Classic STE with reciprocal changes (the one we already knew)
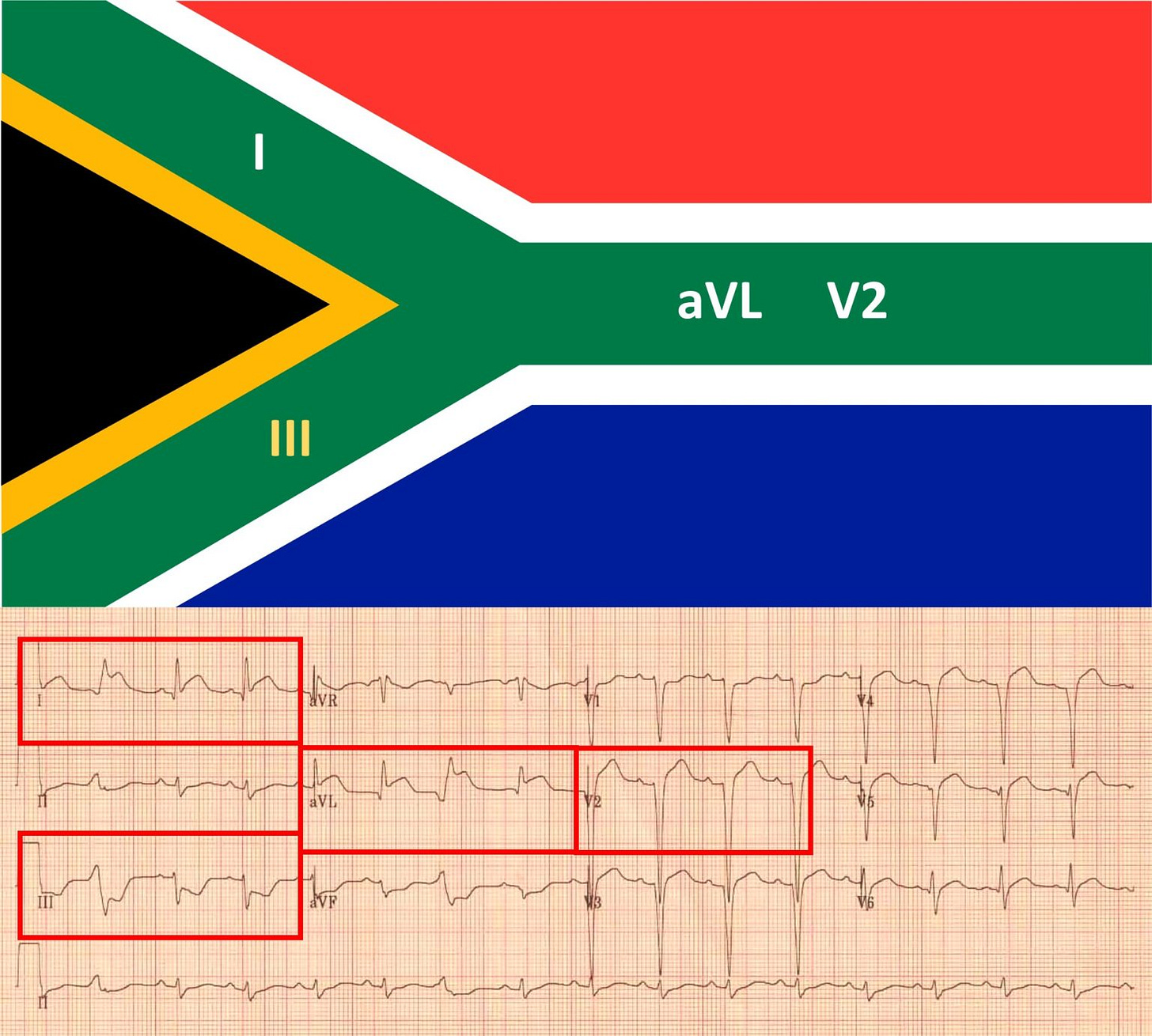
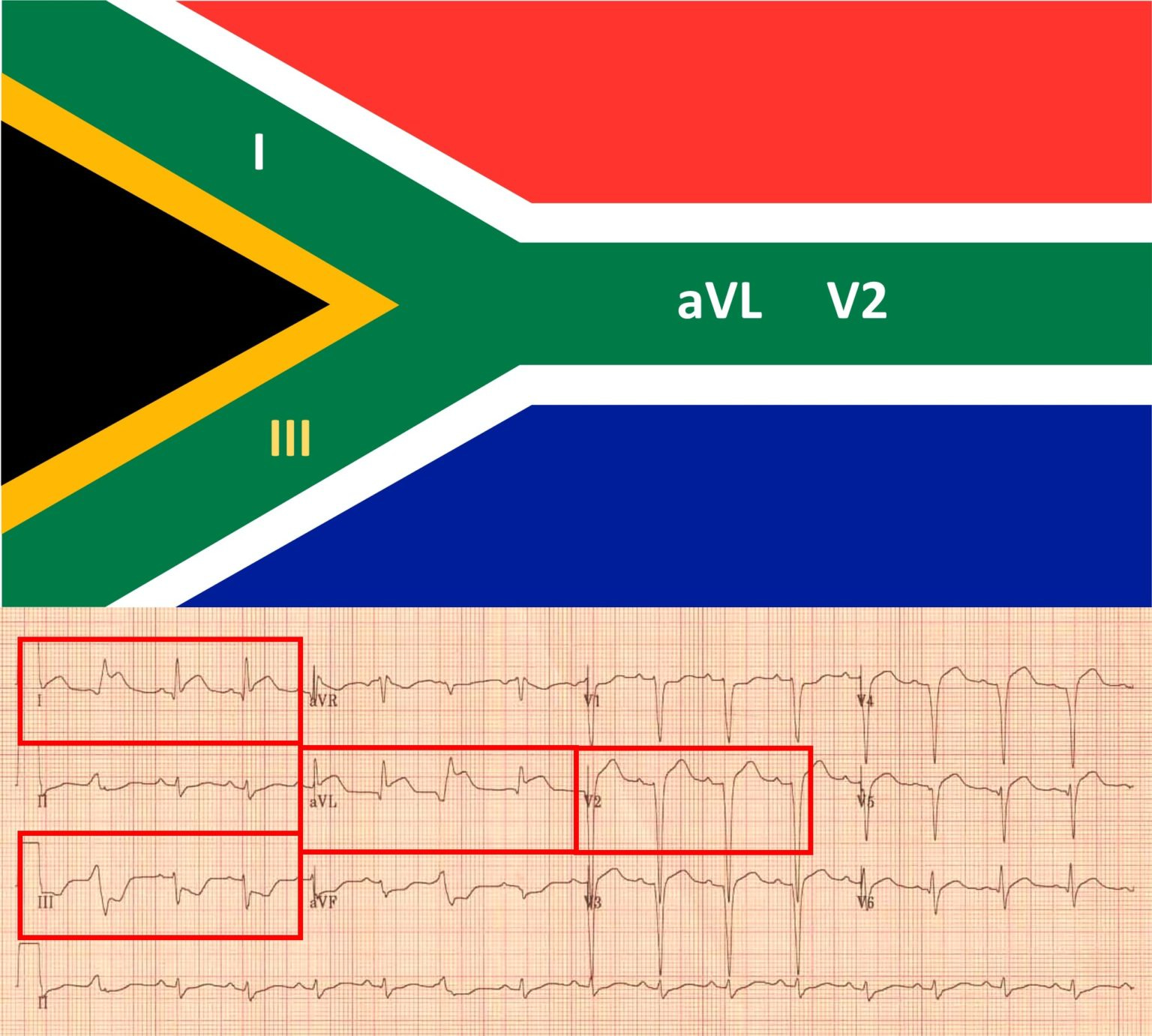
High lateral MI - STE in I and aVL with STD in III/aVF, often subtle STE in V5/V6. The “South African flag sign.” (Image: South Africa Flag sign on ECG | ClinCaseQuest)
Posterior MI
Right ventricular MI
De Winter T-waves
Modified Sgarbossa (LBBB or paced)
The guideline also calls out high-risk patterns that don’t yet meet ACOMI threshold but demand close monitoring and low threshold for angiography:
Wellens T-waves
Diffuse STD with STE in aVR
Hyperacute T-waves
Troponin: Know Your Assay
High-sensitivity assays only. The guideline is unambiguous - hs-cTn enables rapid safe rule-out strategies that conventional troponin simply cannot support.
Key rules:
Use sex-specific 99th percentiles. A single overall cut-off underdiagnoses MI in women.
Serial results must use the same assay. You cannot interpret a delta across different platforms.
Single measurement rule-out requires symptom onset ≥2 hours. If they rolled in within 2 hours, you need serial testing.
In transgender women, use the female (lower) cut-off pending more data.
The guideline recommends either the 0/1-hour or 0/2-hour strategy. Both are validated and use assay-specific thresholds. The key values are summarized in Table 7 of the guideline.
Three-bucket triage applies to all strategies:
low risk (discharge, no further cardiac testing required),
intermediate risk (further evaluation - outpatient if both values ≤99th percentile, inpatient if either elevated), and
high risk (admit).
Most clinicians use a clinical risk score like EDACS or HEART integrated into a pathway with a contemporary troponin assay. hs-cTn-based strategies consistently outperform these in identifying low-risk patients, but they remain the validated fallback where hs-cTn isn’t available.
NSTEACS: Risk-Stratified Timing
Not everyone with a NSTEMI needs a cath lab tonight. But some absolutely do.
Very high risk — within 2 hours:
Haemodynamic instability or cardiogenic shock
Life-threatening arrhythmias
Mechanical complications of MI
Ongoing symptoms with STD >1 mm in ≥6 leads plus STE in aVR/V1, or Wellens on ECG
Recurrent intermittent STE
High risk — within 24 hours:
Confirmed NSTEMI
Dynamic ST/T changes
GRACE score >140
High-risk hs-cTn algorithm result
Lower risk: Consider outpatient non-invasive testing (CTCA preferred for those without known CAD).
Women: Use GRACE 3.0 specifically — GRACE 2.0 underestimates mortality in women. The guideline is explicit on this, and on the need to actively counter the documented disparity in women receiving invasive strategies and radial access.
Older adults: An invasive strategy is reasonable if no significant frailty, multimorbidity, or cognitive dysfunction but should be based on individual assessment. The evidence for benefit is there, but at the cost of higher bleeding risk.
Antiplatelet Therapy
STEMI / NSTEACS with planned PCI:
Aspirin 300 mg loading + ticagrelor or prasugrel (the latter is TGA approved but not on the market yet)
Clopidogrel if on anticoagulation, previous haemorrhagic stroke, or moderate-severe liver disease
STEMI with fibrinolysis:
Aspirin + clopidogrel (not ticagrelor or prasugrel)
Opiates and P2Y12 loading: Both morphine and fentanyl reduce absorption and antiplatelet effect of oral P2Y12 inhibitors in the early ACS phase. Worth knowing, but there is no suggestion of how to get around it in the guideline…
Cardiogenic Shock and Cardiac Arrest
Cardiogenic shock:
Culprit-only PCI. CULPRIT-SHOCK settled this — multivessel PCI at the index procedure increases 30-day mortality.
No routine IABP. Strong recommendation.
No routine VA-ECMO. Strong recommendation.
Impella (percutaneous LVAD): Weak recommendation, consider selectively. DanGer Shock showed reduced mortality in a carefully selected STEMI-shock population, but the benefit came with significantly higher vascular complications (24% vs 6.2%).
Post-arrest:
STE on ECG post-ROSC → emergency reperfusion. Standard.
No STE post-ROSC and haemodynamically stable → no routine emergency angiography. Seven RCTs showed no survival or neurological benefit over a delayed strategy.
The Equity Flag
This guideline is unusually explicit about equity, dedicating specific recommendations to:
Women — chest pain is still the most common presentation (same as men), but misdiagnosis is documented and disparity in invasive management is real. Active vigilance is required.
First Nations peoples — younger, higher risk factor burden, lower intervention rates, worse outcomes. Tailored care and culturally appropriate management are called out throughout.
Older adults — angina equivalents are common. Dyspnoea, fatigue, and dizziness may be the presenting syndrome. Half-dose TNK. Individualize everything.
Regional and remote — pre-hospital fibrinolysis, telehealth ECG interpretation, and telemedicine-supported risk stratification are explicitly supported.
A nice quick refresh, really liked it 👍🏻
Good content! I like the comparison between the American and Australian guidelines. It would be interesting to know why there is a difference in door to balloon time goals between the 2 guidelines. I also found it interesting the point about opiates decreasing absorption of anti platelets early in an AMI. I have not seen in our ED that we give the loading dose ticagrelor or prasugral in ACS. Is there evidence to support it being given in ED, or is it just as effective to start within 24 hours? Thanks for the info, Joe.